Detecting Heart Disease With Intravascular Imaging
Detecting vulnerable plaques is now possible using the latest intravascular imaging technology. We focus on how this can help with early detection of heart disease and prevention of its recurrence.


Transcript
Join us as we explore Medical Frontiers.
The leading cause of death worldwide is heart disease.
This includes myocardial infarction, commonly known as a heart attack,
and angina, a condition characterized by severe chest pain.
These diseases are mainly due to the narrowing and blockage of the heart's blood vessels.
Blood vessel abnormalities can progress unnoticed and develop into diseases that strike unexpectedly.
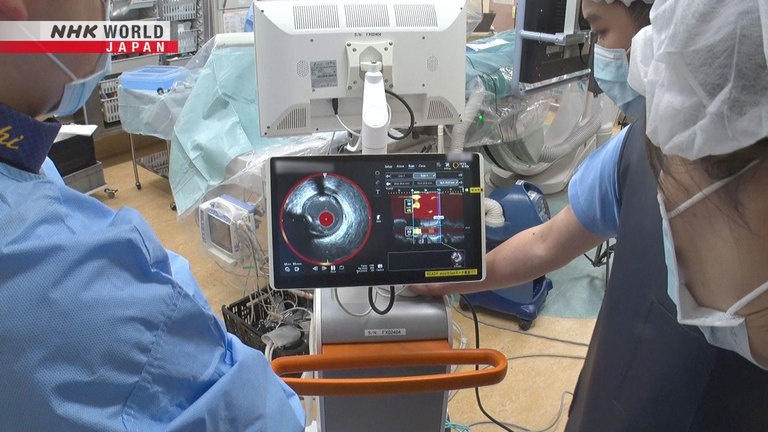
This small device is inserted into the blood vessels to identify the cause of heart attacks,
in a technique known as intravascular imaging.
Today, we'll explore the efforts of doctors working to prevent and treat heart disease
by detecting high-risk conditions within blood vessels at an early stage.
Juntendo University Hospital is a leading medical institution in Japan.
It conducts over 2,000 cardiac catheter examinations and surgeries each year.
A man in his 70s who complained of chest pain was diagnosed with angina.
The condition occurred due to narrowing in a section of his left coronary artery,
leading to insufficient oxygen reaching his heart muscle.
The main cause of blood vessel narrowing is atherosclerotic plaque.
This plaque forms when substances such as LDL cholesterol build up in the blood vessel walls,
creating deposits that narrow the blood vessels and slow down blood flow.
If a plaque ruptures, it can cause thrombosis,
which may lead to a heart attack or other life-threatening disease.
To treat this, a catheter procedure is performed to widen the narrowed blood vessel.
A tube with a diameter of several millimeters called a catheter
is inserted into the blood vessel through the thigh or the wrist.
Then, another tube called a stent is placed in the narrowed part of the blood vessel to widen it.
The typical recurrence rate for heart conditions is around 5 to 15 percent.
But a report from Australia shows that about 50 percent of patients in the Asia-Pacific region
are hospitalized again within a year.
These recurrences are caused by plaques that went unnoticed during surgery.
Dr. Dohi, thank you so much for your time today. It's great pleasure to meet you.
Hello, Erica.
Dohi Tomotaka is a cardiologist at Juntendo University Hospital.
For over a decade, Dohi has been researching ways to accurately assess plaques
using intravascular imaging, in order to prevent heart disease.
I would imagine it's still a big challenge in terms of treatment of heart attacks.
We look at coronary artery plaques
and evaluate their vulnerability.
Vulnerable plaques can cause angina,
myocardial infarction and sudden cardiac death.
There are two kinds of plaques.
One is "stable plaque."
Plaque naturally builds up in blood vessels due to factors such as age and lifestyle.
Stable plaque is very unlikely to rupture.
The problem is the other type, called "vulnerable plaque," or "unstable plaque."
It occurs due to an excessive buildup of lipids in a blood vessel, putting the vessel on the verge of rupture.
If a vulnerable plaque bursts in the coronary artery,
it causes blockage and stops the flow of blood, causing acute myocardial infarction.
These are cross-section images of blood vessels.
Stable plaques have a low lipid content
and are separated from the vessel's inner space by a thick protective layer.
In contrast, vulnerable plaques have more lipids and a thinner protective layer.
The term "vulnerable plaque" was coined by James Muller in 1989 while he was at Harvard University.
For a long time, there was no technology capable of accurately detecting vulnerable plaques.
However, a device created by a Japanese medical-equipment maker is now proving effective in this regard.
It's an intravascular imaging system called NIRS-IVUS,
which combines Near Infrared Spectroscopy with Intravascular Ultra Sound.
The NIRS-IVUS system is attached to the tip of a catheter.
It has two functions.
The IVUS technology uses ultrasound to visualize the internal structure of a blood vessel,
enabling identification of plaque location and size.
It has been in use for some time.
The NIRS technology provides a better understanding of the quality and quantity of lipids in a plaque.
By combining these two technologies, doctors can more accurately identify vulnerable plaques.
We're doing intravascular imaging.
First, Dohi and his team use ultrasound images to find plaques in the coronary arteries.
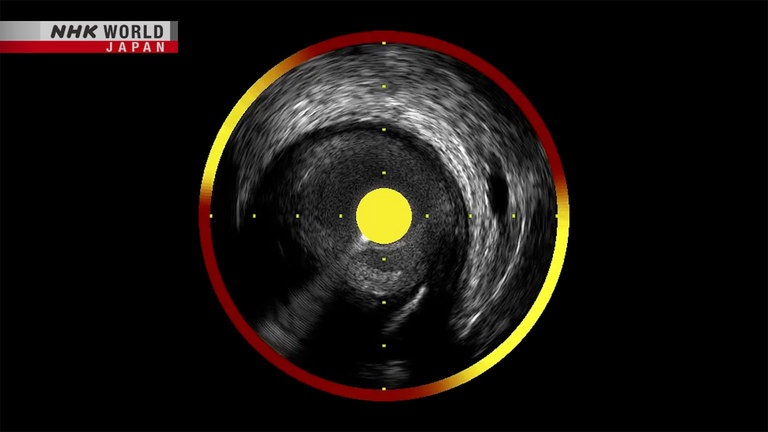
This is an ultrasound image of the inside of a blood vessel, captured by IVUS.
The area circled in blue is the entire blood vessel.
The red part inside it is the inner cavity, where blood flows.
The surrounding area shown in yellow is where plaque is present.
Well...
Bookmark it.
While the ultrasound from IVUS can spot suspicious plaques, it cannot diagnose whether they are vulnerable.
There's a lesion here.
Here's another.
But the narrowing isn't too severe.
The team then uses the near-infrared function of NIRS.
Here, a NIRS image is overlaid on an IVUS image.
Plaque quality is distinguished by color.
Shown in red are the parts without lipid-rich plaques.
In yellow are the sections with lipid-rich plaques.
The condition of plaques is quantified to indicate how unstable they are.
If the number exceeds 400, it is diagnosed as a vulnerable plaque.
As the team continues with intravascular imaging,
they notice a shift from red to yellow in a certain area.
It's turning more yellow here.
The vulnerability index is 475.
Since it exceeds the standard of 400, it is classified as a vulnerable plaque.
This vulnerable plaque is located
slightly before the narrowest point.
The vulnerable plaque was found very close to the narrowest point, where a lesion causing angina was located.
Therefore, Dohi decided to extend the stent by an extra centimeter to reach both the plaque and the lesion.
Without intravascular imaging,
we might have selected a shorter stent.
But the imaging allowed us to treat
both the narrowest part and the plaque.
Following the procedure, the patient no longer feels chest pain and is recovering well.
This man in his 60s suffered sudden chest pain six years ago.
I thought I was going to die. I was scared.
He had developed acute coronary syndrome.
His coronary arteries had narrowed, putting him at risk of myocardial infarction.
He underwent a stent procedure.
Intravascular imaging revealed the presence of a vulnerable plaque in a different location.
The vulnerability index for this plaque was 422, exceeding the standard value of 400.
This vulnerable plaque was found in a different area than the narrowed section of the coronary artery.
In addition, the blood vessel didn't show significant narrowing.
It would have been difficult to diagnose this case using only CT imaging.
Since the vulnerable plaque was found before it ruptured,
the patient was able to start a more proactive treatment.
In this case, Dr. Dohi, what were the patient's, what was, I guess, the root cause of this?
I mean, did he have diabetes or high blood pressure or was?
His susceptibility to coronary artery disease
stems from hypertension and dyslipidemia.
The combination of these risk factors led to
the progress and destabilization of plaques.
It is said that plaques can be stabilized
by lowering lipid levels in the blood.
We enhanced drug therapy,
using medication to reduce lipids.
The patient improved his diet, exercised, and took medication consistently.
As a result, the plaque's vulnerability index dropped from 422 to 106 in two years.
It's been six years, and he has not experienced any recurrences.
The doctor saved my life.
He's like a guardian, keeping my heart beating.
Why is the early detection of unstable plaque so critical?
Early detection enables better
prevention and treatment.
It also changes the patient's mindset,
which is very important.
Recognizing unstable atherosclerosis allows
for more advanced preventive measures.
Sharing imaging results, in particular,
can significantly alter patients' awareness.
But wouldn't this be a great screening test for anyone with, for example,
high triglycerides, high cholesterol and for example, who had issues with imaging?
Wouldn't this be an excellent screening tool?
This is an invasive procedure.
Therefore, it is used for patients who have had
angina or a heart attack to prevent a recurrence.
It is not yet used for people without symptoms.
The development of NIRS-IVUS began when a Japanese company acquired an American firm in 2015.
Japanese doctors helped to develop the system.
US engineers were repeatedly impressed by the Japanese doctors' attention to detail
on aspects such as miniaturization and improvement in image quality.
Working with Japanese doctors is very rewarding.
I think they certainly appreciate the technique and technologies
for what they can do and what they can provide them at treating patients.
They bring a very deep appreciation for how important it is to have all the information,
not just of the vessel, but also the clinical situation in which the images are recorded.
Columbia University's Maehara Akiko, one of the world's leading experts in cardiovascular imaging,
is examining the effectiveness of NIRS-IVUS.
We perform the NIRS-IVUS and we look for like three or four years natural history
and we see NIRS-IVUS can predict future plaque which is causing the event.
So I think like, truly, how we can change the patient's life,
what is efficacy in terms of the treatment standpoint.
That's I think we need more data and that's because it's the biggest challenge.
Dr. Dohi, I mean this is incredibly exciting imaging and technology
but are you working on anything new or what else are you currently working on?
Prevention is crucial. We have accumulated
extensive data from various patients.
We can analyze it to identify individuals
prone to vulnerable plaques.
This can help to prevent myocardial infarction.
It's important to combine data from patients and
imaging to understand and categorize the risks.
In the future, will you be looking at, for example, AI or artificial intelligence, to be able to actually read that data?
I think it's crucial to assess
plaques throughout the entire heart.
The use of AI is essential to ensure we find them.
It's also important not to feel overly reassured
when checkups show everything is normal.
The patient diagnosed with a vulnerable plaque six years ago has been addressing his condition through three aspects:
diet, exercise and medication.
He's paying special attention to his diet.
A blood test before surgery showed that his LDL cholesterol level was 203,
surpassing the hospital's maximum standard of 139.
His triglyceride level was 268, while the maximum standard was 149.
He had both dyslipidemia and hypertension.
I love greasy food, such as
pork cutlet on rice and fried chicken.
Like many middle-aged Japanese men,
I'd eat lots of greasy meat dishes.
He also had a sweet tooth.
His hobby was to try ice cream from various regions of Japan while traveling.
I assumed I was at risk
of developing arterial stiffening.
But I used to work out a lot. I assumed I'd be OK.
I was shocked when I had a heart attack.
Juntendo University Hospital has created guidelines to provide dietary instructions for patients.
Leading the hospital's efforts on nutritional management is Enomoto Mari, a nationally registered dietitian.
What sort of dietary advice was given or dietary guidance was given to the patient?
And also specifically how did you give the advice?
We talked about managing blood pressure,
blood sugar levels and body weight.
These are ways to help reduce visceral fat.
We also explained which fats to avoid.
Our advice focused on these 4 points.
Enomoto recommended that the patient check his weight and Body Mass Index every day.
She says knowing those numbers motivates patients to improve their dietary habits.
To manage his blood pressure, she advised keeping his daily salt intake below 6 grams,
roughly equal to a slightly heaped teaspoon - just like the meals during his hospital stay.
To regulate his blood sugar levels, she suggested reducing carbohydrate intake, even though he wasn't diabetic.
As for fats, she recommended limiting his saturated fats,
commonly found in the fatty parts of meat and dairy products, to less than 15 grams a day.
She also advised avoiding trans fats, often contained in pastries and other sweets.
I tell patients that pastries
are considered sweets, not bread.
I advise them not to replace meals with pastries.
The patient started working diligently to improve his diet.
He says he has become aware of the importance of proper eating.
I eat pork cutlets less often now.
My life is at stake. I have no choice.
The satisfaction of maintaining a healthy
lifestyle also helps to motivate me.
He also took medication.
Two years after heart surgery, his plaque improved, and he achieved a weight loss of five kilograms.
His LDL cholesterol level dropped from 203 to 30, and triglycerides decreased from 268 to 90.
His high blood pressure also showed signs of improvement.
His meals typically include options such as low-calorie soba noodles and a tuna salad.
His dietary habits have changed significantly.
I used to be carefree, but
my illness served as a wake-up call.
I've become cautious in a good way,
ensuring I don't push myself too hard.
I often find myself thinking, "Are you OK?
Take it easy." I'm mindful not to overdo things.
Everyone should take their health seriously.
Preventive steps should be taken to avoid
illness, and this goes beyond medication.
It involves reevaluating lifestyle,
including exercise and dietary habits.
Proactive steps are crucial for a healthy life.
If you don't exercise, doing even a little bit
can have preventive effects.
This is important for a long, healthy life.
Thank you so much. It's been a pleasure having you on the program.
Thank you, Erica.
Today, we explore samurai walking,
a method for covering long distances without feeling tired or straining the body.
In times without modern transportation, the walking style in Japan differed significantly from today.
People would travel the roughly 500 kilometers between Kyoto and what is now Tokyo entirely on foot.
Hello William. It's a great pleasure to meet you.
Pleasure to meet you, Erica.
Our instructor on samurai walking is William Reed.
Reed has lived in Japan for more than 40 years.
He teaches traditional Japanese martial arts and calligraphy at a university.
How do people normally walk? What's the first part of the body to move?
I think the foot and it's usually we think of the heel.
I think everyone's going by, "heel, toe, heel, toe, swing the arms."
- Yes. Swing the arms...
- Yeah. So basically it'll be "heel, toe..."
Normally, we swing our arms widely and lift our toes as we walk.
The way the samurai would walk is, first of all, they don't swing their arms.
And they don't swing their arms and they don't take big strides. They take very small steps.
I mean, of course, they didn't have paved streets and stuff, but they would walk in a vary of small steps.
It's called "komata."
And so it would be like this, you know, they would be walking like this.
The key to samurai walking is to avoid swinging the arms widely,
and to keep the toes down and take small strides.
And you can do it fast, by the way.
But if you just think of Japanese footwear, which is designed, and kimono,
which is designed to help you walk in that way and you take smaller steps.
So how did they really walk? Well,
you can look at traditional arts, even noh and kabuki and also the martial arts.
And what they do is the first part of the body to move is not the foot, it's the tanden.
So, again, we're coming back to the tanden.
Tanden refers to the area just below the navel.
In Oriental medicine, it is considered a gathering point for "ki," or energy.
Being aware of the tanden is important in samurai walking.
Before walking, start by checking your posture using a wall.
Make sure your heels, buttocks, shoulder blades and the back of your head are touching the wall.
Then, take half a step forward, and you'll naturally adopt a comfortable posture.
Now, here's where we start to walk.
Now, instead of taking a step with the foot, you would move your tanden.
- Now that's your pelvis.
- Yes.
An image that might help you in this is think of the pelvis is like a boat and the spine is like a mast.
And you have a sail.
Focus on my tanden.
Just move your pelvis forward and the wind pushes you and we go along,
so you don't have to think about your arms.
You don't have to move your feet with the heel strike.
- It's just natural. Natural.
- Natural. It feels a lot more effortless.
It feels like - I love the image of gliding or floating, and that's what it feels like.
Start walking with an upright posture while focusing on your tanden.
Your body will sway less, and the strain on your lower back and knees will be reduced.
Incorporating samurai walking into your daily life will make walking easy.
It can also motivate you to start regular exercise.
It just feels effortless.
I mean, it feels like we're just gliding, moving along without kind of the head being involved.
It's just... it's a natural movement.
What happens is that once you learn it by body, it becomes natural.
You don't have to think about it. And then you can enjoy nature.
It becomes more visible to you.
Yeah, I can feel my shoulders have actually come down. I feel a lot more relaxed.
It's been a pleasure to work with you. Thank you very much.